Testicular Cancer
Are you a son, brother, father, mother, spouse, or friend of someone who is? Know this: There will be 7.920 new cases of
Testicular Cancer diagnosed * It is
recommended that all men do a monthly testicular self-exam
from puberty to the mid 40's. Newsbytes - Recent stories in the press "Get
a Grip!" Testicular Cancer Awareness Week Campaign
April 1-7
Undecended
Testicle
Testicular
Cancer - What Is It? (Short version.) The reason women statistically outlive
men may have something to do with the idea of survival of
the fittest. Despite the stereotype that men enjoy "getting
physical" more than women, a poll of nearly 15,000 Americans
conducted by Hartsdale, NY-based American Sports Data Inc.
last year found that women engage in more physical fitness
activities than men by a 6 to 4 ratio. (Complete
version.) The
Complete Version Normal body cells grow, divide, and die in an orderly fashion. During the early years of a person's life, normal cells divide more rapidly until the person becomes an adult. After that, normal cells of most tissues divide only to replace worn-out or dying cells and to repair injuries. Cancer cells, however, continue to grow and divide and can spread to other parts of the body. These cells accumulate and form tumors (lumps) that may compress, invade, and destroy normal tissue. If cells break away from such a tumor, they can travel through the bloodstream, or the lymph system to other areas of the body. There, they may settle and form "colony" tumors. In their new location, the cancer cells continue growing. The spread of a tumor to a new site is called metastasis. When cancer spreads, though, it is still named after the part of the body where it started. For example, if prostate cancer spreads to the bones, it is still prostate cancer, and if breast cancer spreads to the lungs it is still called breast cancer. Leukemia, a form of cancer, does not usually form a tumor. Instead, these cancer cells involve the blood and blood-forming organs (bone marrow, lymphatic system, and spleen), and circulate through other tissues where they can accumulate. It is important to realize that not all tumors are cancerous. Benign (noncancerous) tumors do not metastasize and, with very rare exceptions, are not life-threatening. Cancer is classified by the part of the body in which it began, and by its appearance under a microscope. Different types of cancer vary in their rates of growth, patterns of spread, and responses to different types of treatment. That's why people with cancer need treatment that is aimed at their specific form of the disease. In America. half of all men and
one-third of all women will develop cancer during their
lifetimes. Today, millions of people are living with cancer
or have been cured of the disease. The risk of developing
most types of cancer can be reduced by changes in a person's
lifestyle, for example, by quitting smoking or eating a
better diet. The sooner a cancer is found, and the sooner
treatment begins, the better a patient's chances are of a
cure. What is Testicular
Cancer? The testicles (also called the testes; a single testicle is also called a testis) are a part of the male reproductive system. These two organs, each normally somewhat smaller than a golf ball in adult males, are contained with a sac of skin called the scrotum, which hangs beneath the penis. The testicles manufacture the male hormones. The most abundant is testosterone. They also produce sperm, the male reproductive cells. Sperm cells are carried from the testicle by the vas deferens to the seminal vesicles where they are mixed with fluid produced by the prostate gland. During ejaculation, sperm cells, seminal vesicle fluid, and prostatic fluid enter the urethra, the tube in the center of the penis through which both urine and seminal fluid exit the body.  The testicles contain several types of cells, each of which may develop into one or more types of cancer. It is important to distinguish these types of cancers from one another because they differ in their prognosis (outlook for survival) and in the ways they are treated. Germ Cell Tumors Over 90% of cancers of the testicle develop in certain cells known as germ cells. ("Germ" means seed; the term refers to the role of male germ cells in producing sperm cells.) There are two main types of germ cell tumors (GCTs) in men: seminomas and nonseminomas. (The suffix -oma means tumor.) Many testicle tumors contain features of both types. Because of the way these "mixed" tumors grow, spread and respond to treatment, they are classified as being nonseminomas. Most invasive testicular germ cell cancers begin as a noninvasive form of the disease called carcinoma in situ (CIS) or intratubular germ cell neoplasia. Researchers have estimated that it takes about 5 years of CIS to progress to the invasive form of germ cell cancer. When a cancer become invasive, its cells have penetrated the surrounding tissues and may have spread through either the blood circulation or the lymph nodes to other parts of the body. Seminoma: About half of all testicle germ cell cancers are seminomas. They develop from the sperm-producing germ cells of the testicle. There are two main subtypes of these tumors distinguished by their appearance under the microscope: typical (or classic) seminomas and spermatocytic seminomas. Over 90% of seminomas are typical. Most spermatocytic tumors grow very slowly and usually do not metastasize (spread to other parts of the body). The average age of men who are diagnosed with spermatocytic serminoa is 65, about 15 years older then the average age of men with typical seminomas. Nonseminoma Germ Cell Cancer: These cancers tend to develop earlier in life than seminomas, usually occurring in men in their 20s. The main types of nonseminoma germ cell cancers are embryonal carcinoma, yolk sac carcinoma, chorocarcinoma and teratoma. Most tumors are mixed and have at least two different types. This does not change treatment. All nonseminomatous germ cell cancers are treated the same way. This means that the exact type of nonseminomatous testicular cancer a person has is not that important. Embryonal carcinoma: This is a type of nonseminoma germ cell cancer, where the embryonal cell type is most plentiful. It accounts for about 20% of testicle tumors. Seen under a microscope, these tumors can resemble tissues of very early embryos. This type of nonseminoma tends to be aggressive, which means it is likely to metastasize and grow rapidly. Stromal Tumors Tumors can also arise in the supportive and hormone-producing tissues, or stroma, of the testicles. Such tumors are known as gonadal stromal tumors. They account for 4% of adult testicle tumors and 20% of childhood testicular tumors. The two main types are Leydig cell tumors and Sertoli cell tumors. Leydig cell tumors: Leydig cell tumors develop from normal Leydig cells (also called interstitial cells) of the testicle. These are the cells that normally produce androgens (male sex hormones). Leydig cell tumors may develop in adults (75% of cases) or children (25% of cases). They often produce androgens, but in some cases produce estrogens (female sex hormones). Although most Leydig cell tumors do not spread beyond the testicle and are cured by surgical removal, a small number metastasize (spread to other parts of the body). Metastatic Leydig cell tumors have a poor prognosis, since they do not respond well to chemotherapy or radiation therapy. Secondary Testicular Tumors Secondary testicular tumors are those which start in another organ and then spread to the testicle. Lymphoma is the most common secondary testicular cancer. Among men over 50 years to age, testicular lymphoma is more common than primary testicular tumors. Their prognosis depends on the type and stage of lymphoma. The usual treatment is surgical removal, followed by radiation and/or chemotherapy. Cancers of the prostate, lung, skin
(melanoma), kidney, and other organs can secondarily spread
to the testicles. The prognosis for these cancers is usually
poor because these cancers generally spread widely to other
organs as well. Treatment depends on the specific type of
cancer. What are the key
statistics about testicular cancer? Testicular cancer is one of the most curable forms of the disease. Studies show that the cure rate exceeds 90% in all stages combined. The 5-year survival rate for stage 1 and stage 11 testicle cancer is more than 95%. The 5-year survival rate for stage 111 disease, in which cancer has spread beyond local lymph nodes, is 75%. The 5-year survival rate refers to the
percent of patients who live at least 5 years after their
cancer is diagnosed. Many of these patients live much longer
than 5 years after diagnosis, and 5-year rates are used to
produce a standard way of discussing prognosis. Five-year
relative survival rates exclude from the the
calculations patients dying of other diseases, and are
considered to be a more accurate way to describe the
prognosis for patients which a particular type and stage of
cancer. Of course, 5-year survival rates are based on
patients diagnosed and initially treated more than 5 years
ago. Improvements in treatment often result in a more
favorable outlook for recently diagnosed patients. What are the risk
factors for testicular cancer? Age: Most testicular cancers occur between the ages of 12 and 50. But, this cancer can affect males of any age, including infants and elderly men. Cryptorchidism: The main risk factor for testicular cancer is a condition called cryptorchidism or undescended testicle(s). This term comes from the Greek words kryptos meaning hidden and orchis meaning testicle. In a fetus, the testicles normally develop inside the abdomen and descend into the scrotum before birth. In about 3% of boys, however, the testicles do not make this descent. Sometimes the testicle remains in the abdomen; in other cases, the testicle starts to descend but remains stuck in the groin area. About 14% of cases of testicle cancer occur in men with a history of cryptorchidism. The risk of testicle cancer is somewhat higher for a testicle that was positioned in the abdomen, as opposed to one that descended at least part way. In men with a history of cryptorchidism, most cancers develop in the testicle that did not descend, but up to 25% of cases occur in the normally descended testicle. Based on these observations, some doctors conclude that cryptorchidism is not the direct cause of testicular cancer, but that some other disorder is responsible for increasing the testicular cancer risk and preventing normal positioning of one or both testicles. Most cryptorchid testicles will eventually descend on their own in the child's first year. Sometimes a surgical procedure known as orchiopexy is necessary to bring the testicle down into the scrotum. Some experts believe that performing orchiopexy before puberty may reduce the risk of developing certain types of germ cell tumors. Family history: A family history of testicular cancer increases the risk. If one man has the disease, there is an increased risk that one or more of his brothers will also develop it. A recent study, found that nonseminoma germ cell tumors occur more frequently among men with certain occupations (Miners, oil and gas workers, leather workers, food and beverage processing workers, janitors, and utility workers). It may be that exposure to certain chemicals contributes to development of the disease. Studies have not yet identified any specific chemicals as being responsible. No association was found between occupation and risk of seminoma tumors. One study found a slightly higher risk of germ cell tumors among men with prolonged occupational exposure to extremely hot or cold temperatures. However, these occupational associations need to be confirmed in other studies before it can be concluded they represent a significant component of testicular cancer risk. Injury: There is no convincing evidence that injury to the testicles increases the risk of developing cancer. HIV Infection: There is some evidence that men infected with the human immunodeficiency virus (HIV), particularly those with AIDS, are at increased risk. No other infections have been shown to increase testicular cancer risk. Carcinoma in situ: This condition does not produce a mass or cause any symptoms. Carcinoma in situ (CIS) in the testicles almost always progresses to cancer. In some cases, CIS is detected in men who undergo a testicular biopsy during medical evaluation of infertility. Cancer of the other testicle: A history of testicle cancer is another risk factor. Men who have been cured of cancer in one testicle have an increased risk of developing cancer in the other testicle. Race and ethnicity: The risk of testicular cancer among white American men is about five times that of African-American men and more than double that of Asian-American men. The risk for Latinos is intermediate between that of Asians and non-Latino whites. The reason for this different is not known. Testicular cancer risk has more than doubled among white Americans in the past 40 years, but has remained the same for African-American men. Worldwide, the risk of developing this disease is highest among men living int the US, the UK and Scandinavia, and lowest among African and Asian men. Maternal hormone use: Although men whose mothers took the synthetic estrogen diethylstilbestrol (DES) during pregnancy have an increased risk of certain congenital (present at birth) reproductive system malformations, there is no convincing evidence that DES exposure significantly increases a man's risk of developing testicle cancer. Vasectomy: Some earlier
studies raised the possibility that vasectomy (an
operation to produce sterility) might increase the risk of
testicle cancer. However, recent studies have not found any
increased risk among men who have had this operation. Do we know what
causes testicular cancer? During the past few years, researchers have learned much about certain changes in chromosomes and DNA that may be responsible for causing normal testicular germ cells to develop into germ cell tumors. Chromosomes are microscopic pieces of DNA and protein that carry genetic information about inherited traits. Each sperm or egg cell has half as many chromosomes as other body cells. So, when the sperm and egg combine, the resulting fetus has a normal number of chromosomes - half of which are from each parent. This is why we tend to resemble our parents. Meiosis is the process by which
germ cells with 46 chromosomes develop into sperm or egg
cells with 23 chromosomes. There is evidence that testicular
germ cell tumors may form when something abnormal happens
during meiosis. Instead of forming normal sperm cells with
23 chromosomes, all 46 chromosomes remain. Usually, these
chromosomes become unstable and progressively more abnormal
in their shape and number (which is often between 69 and
82). Changes to chromosome 12 are particularly common, and
scientists are studying DNA from this chromosome to learn
more about exactly what goes wrong during meiosis and how
this might be prevented or reversed. Can testicular cancer
be prevented? Can testicular cancer
be found early? Signs and Symptoms of Testicle Cancer In about 90% of cases,men have a painless or an uncomfortable lump on a testicle, or they may notice testicular enlargement or swelling. Men with testicular cancer often report a sensation of heaviness or aching in the lower abdomen or scrotum. In rare cases, men with germ cell cancer notice breast tenderness or breast growth. This symptom results from the fact that certain types of germ cell tumors secrete high levels of a hormone called human chorionic gonadotropin (HCG), which affects breast development. Blood tests can measure HCG levels; these tests are important in diagnosis, staging, and in follow-up of some testicular cancers. Testicular Leydig cell tumors and Sertoli cell tumors often result in a mass that can be distinguished from a germ cell tumor only by examination of the tumor under a microscope. However, come Sertoli cell or Leydig cell tumors produce androgens (male sex hormones) or estrogens (female sex hormones). These hormones may cause symptoms that provide clues to the correct diagnosis. Estorgen-producing tumors may not cause any specific symptoms in men, but in boys they can cause growth of facial and body hair at an abnormally early age. Even when testicular cancer has spread to other organs, only about 1 man in 4 may experience symptoms related to the metastases prior to diagnosis. Lower back pain is a frequent symptom of later-stage testicle cancer. If the cancer has spread to the lungs and is well advanced, shortness of breath, chest pain, cough, or bloody sputum may develop. Some men with testicular cancer have no symptoms at all, and their cancer is found during medical testing for other conditions. Sometimes, imaging tests done to find the cause of infertility can uncover a small testicular cancer. Or, testicular biopsies to evaluate infertile men may find carcinoma in situ. There are a number of noncancerous conditions, such as testicle injury, that can produce symptoms similar to those of testicle cancer. Inflammation of the testicle, known as orchitis, can cause painful swelling. Causes of orchitis include viral or bacterial infections. About 1 man in 5 who contracts mumps as an adult experiences orchitis in one or both testes. If you have any of the sings or symptoms described above, discuss them with your doctor without delay. Remember, the sooner you receive an accurate diagnosis, the sooner you can start treatment and the more effective your treatment will be. Testicular Examination Doctors agree that examination of a man's testicle is an important part of a general physical examination. The American Cancer Society includes testicular examination in its recommendations for routine cancer-related checkups. The issue of regular testicular self-examination is more controversial. The American Cancer Society believes it is important to make men aware of testicular cancer and remind them that any testicular mass should be evaluated by a doctor without delay. Some doctors feel that delay in seeking medical attention after discovering a mass is the most common reason for a delay in treatment. Other doctors feel that not noticing masses promptly is also an important factor in delaying treatment and they recommen monthly testicular self-examination by all men after puberty. The ACD does not feel that men with average testicular cancer risk, there is any medical evidence to suggest that monthly examination is any more effective than simple awareness and prompt medical evaluation. However, the choices of whether or not to perform this examination should be made by each man, so instructions for testicular examination are included in this section. Because men with certain risk factors (cryptorchidism, previous germ cell tumor on one side or a family history) have an increased risk of developing testicular cancer, monthly examinations should be seriously considered for these men and the ACS suggests they discuss this issue with their doctor. If you plan to perform the self-exam
the best time to do so is during or after a bath or shower,
when the skin of the scrotum is relaxed. Stand in front of a
mirror and hold the penis out of the way. Examine each
testicle separately. Hold the testicle between the thumbs
and fingers with both hands and roll it gently between the
fingers. Look and feel for any hard lumps or nodules (smooth
rounded masses) or any change in the size, shape, or
consistency of the testes. Contact your doctor if you detest
any troublesome signs. Be aware that the testicles contain
blood vessels, supporting tissues, and tubes that conduct
sperm; some men may confuse these with cancer. If you have
any doubts, ask your doctor. (Editor: We see no medical
risk in self-examinations and provide more detail on
self-exams in English
and Spanish
elsewhere. ) How is testicular
cancer diagnosed? History and physical exam: The first step is for the doctor to take a complete medical history to check for risk factors and symptoms. During a physical exam, the physician will feel the testicles to detect any sign of swelling or tenderness, and the size and location of any mass. The doctor will also examine the abdomen to feel for enlarged lymph nodes which are a sign that the cancer has spread to the retroperitoneal lymph nodes (lymph nodes found in the back of the abdomen). Ultrasounds: If a mass or nodule is present, the physician will probably want to see an ultrasound image of the testicle to help decide if it is likely to be a cancer. Ultrasound uses sound waves to create "echoes" of internal organs. The pattern of echoes reflected by tissues can be useful in distinguishing hydrocele (a fluid accumulation around the testicle) and certain benign masses from cancers. If the tumor is solid, then it is probably cancer. Blood tests: Certain blood tests are sometimes helpful in diagnosing testicular tumors. Some testicle cancers secrete high levels of certain proteins such as alpha-fetoprotein (AFP), human chorionic gonadotropin (HCG), or placental alkaline phosphatase (PLAP). The tumors may also increase the levels of enzymes such as lactate dehydrogenase (LDH). Nonseminomas often raise AFP levels, while seminomas do not. LDH, HCG, and PLAP levels are increased in some seminomas and nonseminoma germ cell testicle cancers. These substances are not produced by Sertoli or Leydig cell tumors. Blood tests can measure the levels of these substances present in the serum (the fluid portion of blood). These proteins are not usually elevated in the plasma if the tumor is small. Therefore, these tests are also useful in estimating how much cancer is present, predicting a patient's prognosis, and evaluating the response to therapy to make sure the tumor has not returned. Surgery: If a suspicious growth is found, a surgeon will need to remove the tumor and send it to the laboratory. There a pathologist (a doctor specializing in laboratory diagnosis of diseases) looks at this tissue under a microscope. If cancer cells are present, the pathologist sends back a report describing the type and extent of the cancer. Whenever possible, surgeons try to remove the entire tumor together with the testicle and spermatic cord. Eachspermatic cord contains one vas deferens, a tube through which sperm cells reach the seminal vesicles for storage until ejaculation. Even more importantly, the spermatic cord contains blood and lymph vessels that may act as a pathway for testicle cancer to spread to the rest of the body. The operation is done through an incision in the inguinal (groin) area. This surgical strategy minimizes the risk that cancer cells will spread during the operation. In rare cases, when a diagnosis of
testicle cancer is uncertain, the doctor may perform a
biopsy before removing the testicle. During this operation,
the surgeon makes an incision in the groin, withdraws the
testicle from the scrotum, and examines it without cutting
the spermatic cord. If suspicious tissue is seen, a portion
of the tissue is removed and immediately examined by the
pathologist. If cancer is found, the testicle and spermatic
cord are removed. If the mass is not cancerous, the testicle
can often be returned to the scrotum and treatment will
involve surgery to remove only the mass or the use of
appropriate medications. How is testicular
cancer staged? Examinations and Tests for Staging Testicle Cancer Computed tomography (CT): This test uses a rotating x-ray beam to create a series of pictures of the body from many angles. A computer processes the information provided by the scan and produces a detailed cross-sectional image of the selected part of the body. To highlight details on at CT scan, a dye may be injected into a vein. The CT scan is especially valuable for identifying the spread of tumors to the lymph nodes. Lymphangiography: In this procedure, a special dye is injected into a lymph vessel and is carried to the lymph nodes. Lymph nodes are a network of bean-sized collections of white blood cells that fight infection. Enlarged lymph nodes could be a sign of a spreading cancer or that your body is fighting an infection. During lymphangiography, a special viewing monitor displays x-ray images of the lymph system which doctors can study to detect signs that cancer has metastasized. CT scans have replaced lymphangiography in staging most cases of testicle cancer. However, the technique is sometimes used for patients in whom early stage nonseminomas have been diagnosed and who are being observed to watch for signs of progression before more chemotherapy or radiation begins. Magnetic resonance imaging (MRI): This technique uses magnetic fields and radio waves instead of x-rays to create images of selected areas of the body. These images can show enlarged lymph nodes and abnormal nodules in certain organs that may indicate spread of cancer from the testicles. MRI is not routinely done as part of a work-up for testicle cancer because CT scans can produce the same information at a lower cost. Other tests: Chest x-rays, bone scans, and other tests also may be performed if metastasis is suspected. Also, blood tests for the proteins AFP, HCG, and LDH will be performed. The TNM Staging System A staging system is a way for the cancer care team to summarize and describe the extent of a patient's cancer. Testicular cancer is staged using a system created by the American Joint Committee on Cancer (AJCC) and the International Union Against Cancer (UICC) called the TNM system. The TNM system of staging contains four key pieces of information: T refers to the extent of spread of the primary tumor to tissues next to the testicle The numbers 0 through 4 appear after T, N, and M to provide more details about each of these factors. The possible values for T are: TX: Primary tumor cannot be assessed The possible values for N are: NX: Regional (nearby) lymph nodes cannot be assessed. The possible values for M are: MX: Presence of distant metastasis cannot be assessed. The possible values for S are: For the purpose of selecting treatment, staging of testicular cancer is sometimes simplified to the following classification: Stage 0: (carcinoma in situ: Preinvasive germ cell cancer Stage 1: No spread to lymph nodes or distant organs Stage II: The cancer has spread to regional lymph nodes but not to lymph nodes in other parts of the body or to distant organs. Non-bulky stage II: There is no spread to retroperitoneal (behind the abdominal cavity) lymph nodes larger than 5 cm (2 inches). Stage III: The cancer has spread to nonregional lymph nodes and/or distant organs, such as the lungs or live. Non-bulky stage III: Metastases are limited to lymph nodes and lungs and no mass is larger than 2 cm (about 3/4 inch) Recurrent: Recurrent
disease means that the cancer has come back (recurred) after
removed during surgery) or in another part of the body. How is testicular
cancer treated? After the cancer is found and staged, your cancer care team will discuss treatment options (choices) with you. It is important to take time and think about all of the choices. In choosing a treatment plan, factors to consider include the type and stage of the cancer as well as your overall physical health. It is often a good idea to seek a second opinion. A second opinion can provide more information and help you feel good about the treatment plan that is chosen. Some insurance companies require a second opinion before they will agree to pay for treatments. The three main methods of treatment for testicular cancer are surgery, radiation therapy and chemotherapy. Surgery Surgery for testicular cancer involves removal of the testicle (or testicles) containing the cancer. An incision is made in the groin and the testicle is withdrawn from the scrotum through the opening. A cut is made through the spermatic cord that attaches the testicle to the abdomen. This procedure is known as a radical inguinal orchiectomy. Special precautions are taken during surgery to avoid spreading cancer cells into the surgical wound or dislodging them from the tumor in the bloodstream. Depending on the type and stage of the cancer, some lymph nodes may also be removed at the same time or during a second operation. This operation, called retroperitoneal lymph node dissection can be a major operation. A large incision is often made in order to remove the lymph nodes. Approximately 10% of patients have temporary complications after surgery such as bowel obstruction or wound infections. Alternatively, in some cases the surgeon can remove lymph nodes through a very small skin incision in the abdomen by using a laparoscope (a narrow lighten tube). If both testicles are removed, no sperm cells will be produced and a man become infertile (unable to father children). Surgery to remove retroperitoneal lymph nodes may cause damage to nearby nerves that control ejaculation. Damage to these nerves may also cause infertility. In order to preserve fertility, surgeons have developed a type of retroperitoneal lymph node surgery that has a better chance of preserving the nerves (nerve-sparing surgery). The success rate in expert hands is 98%. Testicle cancer often affects men who may still be trying to start a family or have more children. These men may wish to discuss nerve-sparing surgery with their doctors, as well as sperm banking (storing frozen sperm cells obtained before treatment). Sexual Impact of Loss of One or Both Testicles Testicles are as symbolic of manhood as breasts are of womanhood. Although some men are not upset about their new appearance, others fear a partner's reaction. This is particularly true of men who are single. In men with testicular cancer, the surgeon usually removes only the abnormal testicle. Very few men ever develop a second tumor in the other testicle. Since the operation also removes the cord above the testicle, that side of the scrotum does look and feel empty. Men with testicular cancer are usually young. They may be single and dating, or they may be athletic and feel embarrassed by the missing testicle when playing sports or in locker rooms. To restore a more natural look, a man can have a testicular prosthesis surgically implanted in his scrotum. The prosthesis is filled with silicone gel, and it comes in many sizes to match the remaining testicle. When in place, it looks and feels like a testicle. The only evidence left of the operation is the scar, which is often partly hidden by pubic hair. When part of the scrotal skin must be removed, a testicular prosthesis may not be able to make the scrotum look normal. Radiation Therapy. Radiation therapy uses a beam of high-energy rays (such as gamma rays or x-rays) or particles (such as electrons, protons, or neotrons) to destroy cancer cells or slow their rate of growth. In treating testicle cancer, radiation is used mainly to kill cancerous cells that have spread to lymph nodes. Radiation therapy for testicle cancer is delivered by a carefully focused beam of radiation from a machine outside the body. This is known as external beam radiation. The main drawback of this method is that the radiation also can destroy nearby healthy tissue along with the cancerous cells. Although uncommon, some men experience a skin reaction that is like a sunburn on the outside of their skin. This slowly fades away. Other possible side effects include fatigue, nausea or diarrhea. To reduce the risk of side effects, doctors carefully figure out the exact does you need and aim the beam as accurately as they can to hit the target. Generally, treatment of testicle cancer involves the use of lower doses than are needed for other types of cancer. Special protective devices will be placed over the remaining testicle to preserve fertility. Chemotherapy Chemotherapy is the use of drugs for treating cancer. The drugs can be swallowed in pill form or they can be injected from a needle into a vein or muscle. Chemotherapy is considered "systemic therapy." This means that the drug enters the bloodstream and circulates throughout the body to reach and destroy the cancer cells. Chemotherapy is an effective way to destroy any cancer cells that break off from the main tumor and travel in the bloodstream to lymph nodes or distant organs. Some types of chemotherapy kill cancer cells directly. Other drugs act by making the cells more vulnerable to radiation. Often the use of two or more drugs is more effective than any single drug. The main drugs used to treat testicle cancer are cisplatin, vinblastine, bleomycin, cyclophosphamide, etoposide, and ifosfamide. These drugs are used in various combinations. Drugs used in chemotherapy can also affect some of the normal, healthy cells in your body, causing side effects. Rapidly growing cells, such as the blood-producing cells of bone marrow, the cells of hair follicles, and the lining of the digestive tract are particularly sensitive to chemotherapy. Among the possible side effects are:
If you have side effects, your cancer care team can suggest steps to ease them. For example, there are drugs available to help control and prevent nausea and vomiting. Fortunately, most side effects will disappear when your course of treatment ends. Some of the drugs used to treat testicular cancer can cause long-term side effects, including kidney damage, damage to small blood vessels causing sensitivity to cold temperatures, nerve damage causing numbness and abnormal tingling, hearing loss, and lung damage causing shortness of breath and reduced capacity for physical activity. Development of a second cancer (usually leukemia) is a very serious but, fortunately a rare side effect. It occurs in less than 1% of testicular cancer patients treated with chemotherapy. Stem Cell Transplantation Studies are being conducted to explore whether high-dose combination chemotherapy with stem-cell transplantation may be valuable in treating some patients with advanced germ cell cancer. In this treatment, blood-forming cells called stem cells are removed from the patient's bone marrow or filtered from the bloodstream using a special machine. These stem cells are preserved by freezing while the patient receives high-dose chemotherapy. One complication of this chemotherapy is destruction of the patient's bone marrow stem cells. As a result, the patient is unable to produce infection-fighting white blood cells, platelets, and red blood cells needed to carry oxygen throughout the body. Although these complications would otherwise be fatal, they can be overcome by returning the frozen cells to the patient after chemotherapy. This allows doctors to use extra high doses of chemotherapy that might increase the likelihood of curing some testicular cancers. Clinical trials Studies of promising new or experimental treatments in patients are known as clinical trials. A clinical trial is only done when there is some reason to believe that the treatment being studied may be of value to the patient. Treatments used in clinical trials are often found to have real benefits. There are three phases of clinical trials in which a treatment is studied before the treatment is eligible for approval by the Food and Drug Administration (FDA). The purpose of a Phase I study is to find the best way to give a new treatment and how much of it can be given safely. Physicians watch patients carefully for any harmful side effects. The research treatment has been well tested in laboratory and animal studies, but the side effects in patients are not completely predictable. Phase II trials determine the effectiveness of a research treatment after safety has been evaluated in a Phase I trial. Patients are closely observed for an anticancer effect by careful measurement of cancer sites present at the beginning of the trial. In addition to monitoring patients for their response, any side effects are carefully recorded and assessed. Phase III trials require entry of large numbers of patients. Some trials enroll thousands of patients. One of the groups may receive standard (the most accepted) treatment, so the new treatments can be directly compared. The group that receives the standard treatment is called the "control group." For example, one group of patients (the control group) may receive the standard chemotherapy for a certain type of cancer, while another patient group may receive a different type of chemotherapy that may or may not contain an investigational drug to see if this improves survival. All patients in Phase III trials are monitored closely for side effects and treatment is discontinued if the side effects are too severe. Researchers conduct studies of new treatment to answer the following questions:
However, there are some risks. No one involved in the study knows in advance whether the treatment will work or exactly what side effects will occur. That is what the studies designed to discover. Wile most side effects will disappear in time, some can be permanent or even life-threatening. Keep in mind that even standard treatments have side effects. Depending on many factors, a patient may decide that a clinical trial will be beneficial. Enrollment in any clinical trial is completely up to you. Your doctors and nurses will explain the study to you in detail and will give you a form to read and sign indicating your desire to take part. This process is known as giving your informed consent. Even after signing the form and after the clinical trial begins, you are free to leave the study at any time for any reason. Taking part in the study does not prevent you from getting other medical care you may need. To find out more about clinical trials, ask your cancer care team. Among the questions you should ask are:
Treatment Options by Stage Stage I Germ Cell Cancers Stage I seminomas are usually treated with radical inguinal orchiectomy (surgical removal of the testicle and spermatic cord) followed by radiation aimed at regional lymph nodes (inguinal and retroperitoneal lymph nodes). Because seminoma cells are very susceptible to radiation, moderate doses of radiation can be used. More than 95% of stage I seminomas can be cured this way. The doctor may recommend radiation therapy even if there is no evidence from the CT scan that the cancer has spread to the nodes. This is because in approximately 15% of cases the testicle cancer of this type, cancerous cells have in fact spread but were not detected during imaging studies. Radiation therapy is usually successful in destroying these hidden (occult) metastases. An alternative approach to treating men with stage I seminomas is currently being evaluated. Instead of treating regional lymph nodes with radiation right after surgery, patients are followed closely with blood tests and regularly scheduled imaging studies for several years. If these tests do not find any evidence of metastasis (spread) beyond the testicle, no additional treatment is given. If metastasis is detected later, radiation or chemotherapy can still be effectively used. This approach is about as effective as immediate radiation therapy, particularly if the original testicle cancer was not larger than 6 cm (about 2 1/2 inches). Stage I nonseminoma germs cell cancers are also highly curable, but the standard approach is different from treatment of seminomas. The initial treatment is radical inguinal orchiectomy. There are then three options:
Stage II Germ Cell Cancers Stage II seminomas and nonseminoma germ cell cancers can be cured in 90-95% of cases. For purposes of treatment, stage II seminomas are classified as either "bulky" or "non-bulky". Bulky refers to the size of the retroperitoneal lymph nodes. Nonbulky cancer is treated with radical inguinal orchiectomy followed by radiation to the regional (retroperitoneal) lymph nodes. Men with bulky tumors undergo radical inguinal orchiectomy, after which they either undergo radiation therapy or retroperitoneal lymph node as well as the more distant abdominal and pelvic lymph nodes, or being a course of combination chemotherapy, which includes cisplatin. Stage II nonseminomatous germ cell tumors are also divided into "nonbulky" and "bulky." For nonbulky disease radical inguinal orchiectomy is followed by retroperitoneal lymph node removal. About one-fourth of these men will not have cancer in their lymph nodes even though their CT scan suggested they might. For the other three-fourths who do have cancer in their lymph nodes, there are two options:
Men with bulky disease in their lymph nodes should, of course, have the testicular tumor removed surgically. But for these men, the next step is not surgery, but chemotherapy. Several regimens are used but the most common contain etoposide, bleomycin, and cisplatin. These are given as three or four courses. Following this, a repeat CT scan will be performed to determine if the retroperitoneal lymph nodes are still enlarged. If they are, a retroperitoneal lymph node dissection will be performed. This is a little harder on men who have had chemotherapy than those who have not. Stage III Germ Cell Cancers Stage III seminomas are treated with surgery followed by chemotherapy with a combination of drugs. The main regimens are the same as those used for stage II testicle cancers (usually etoposide, cisplatin, and bleomycin). This approach produces a cure in over 70% of cases. Those who are not cured might consider enrolling in clinical trials. Patients whose cancer has metastasized to the brain usually receive chemotherapy plus radiation therapy aimed at the brain. Stage III nonseminomas usually receive the same treatment with chemotherapy and have similar survival rates as seminomas. Once chemotherapy is complete, the doctor looks for any cancer that remains. Sometimes a few tumors remain. These are most often in the lung or in the retroperitoneal lymph nodes. Removing these surgically may be curative. Recurrent Germ Cell Cancer Treatment of recurrent germ cell cancer depends on the initial stage and treatment. Retroperitoneal lymph node recurrence after orchiectomy alone for early stage tumors can be treated by surgery if the recurrence is small. Depending on the results of the surgery, chemotherapy may be recommended. If there is extensive retroperitoneal disease or the recurrence is elsewhere, then chemotherapy will be recommended. Tis may be followed by surgery. If a man develops a recurrence after chemotherapy then he will be treated with "salvage chemotherapy" that uses different drugs, typically ifosfamide, cisplatin, and either etoposide or vinblastine. Recently, many men whose disease comes back after chemotherapy are being treated with high-dose salvage chemotherapy followed by autologous bone marrow or peripheral blood stem cell transplantation. For men with recurrent disease, this may be an option rather than standard chemotherapy. ( See the section on "Stem Cell Transplantation" for more information.) Sertoli Cell and Leydig Cell Tumors Radical inguinal orchiectomy is
usually recommended for these types of tumors. Radiation
therapy and chemotherapy are generally not effective in
these rare types of testicle tumor. If metastasis beyond the
testicle is suspected, retroperitoneal lymph nodes may be
surgically removed. What should you ask
your doctor about testicular cancer?
You will no doubt have other questions
about your own personal situation. Be sure and write your
questions down so you remember to ask them during each visit
with your cancer care team. Keep in mind, too, that doctors
are not the only ones who can provide you with information.
Other health care professionals, such as nurses and social
workers, may have the answers to your questions. What happens after
treatment for testicular cancer? Remember that your body is unique and so are your emotional needs and your personal circumstances. In some ways, your cancer is like no one else's. No one can predict precisely how you will respond to cancer or its treatment. Statistics can paint an overall picture, but you may have special strengths such as a healthy immune system, a history of good nutrition, a strong family support system, or a deep spiritual faith. All of these have an impact on how you cope with cancer. Follow-up care is important after treatment. Your health care team will explain what tests you need and how often they should be done. You will need blood tests to measure levels of certain protein markers (alpha-fetoprotein, AFP; human chorionic gonadotropin, HCG; lactate dehydrogenase, LDH) to help detect relapse as early as possible. You will also need x-rays, CT scans, and other imaging studies to detect recurrence, metastasis, or a new tumor. Make a special effort to keep all appointments with your cancer care team and follow their instructions carefully. Report any new or recurring symptoms to your doctor right away. There is about a 1% chance that men who have had cancer in one testicle will develop cancer in the other. Usually this is a new cancer and is not metastasis from the previous tumor. Because testicular cancer or its treatment can make a man infertile, before treatment starts men who wish to father children may want to consider depositing sperm in a sperm bank for later use. Be aware, however, that in many cases the disease can cause low sperm counts, which may make it hard to obtain an adequate specimen. In some cases, if one testicle remains, fertility returns temporarily or permanently following successful treatment for testicle cancer. Typically, for example, fertility returns two years after chemotherapy stops. You may feel that it is worthwhile to explore alternative treatments offered by therapists who are not medical doctors. Before changing your treatment or adding any alternative therapy to your regimen, talk it over with members of your cancer care team. They may have additional information to give you. Cancer treatment can make you feel tired. Give yourself time to recover. Don't feel you have to rush back to work or resume all of your normal activities right away. Give your body the adequate rest it needs and you will feel better in the long run. Do as much as you can to help yourself stay healthy and active. If you smoke, try to quit. Ask your health care team for suggestions about how to quit smoking. Eat a balanced diet of healthy foods, including plenty of fruits, vegetables, and whole grains. Once you get your strength back, try to exercise a few hours each week. Your care providers can suggest the types of exercise that are right you you. Your health care team can suggest
other organizations that might help you during your recovery
from treatment. There are many support groups available that
provide emotional support, friendship, and understanding.
(Resources.) What's new in
testicular cancer research and treatment? Scientists are studying the changes DNA of testicular cancer cells, to learn more about the causes of this disease with the expectation that improved understanding will lead to even more effective treatment. Clinical trials have refined doctors' approaches to treating these cancers and are expected to answer additional questions. For example, studies have identified factors to help predict which patients have a particularly good prognosis and may not need lymph node survey or radiation therapy. On the other hand, studies have found unfavorable prognostic factors that suggest certain patients may benefit from more intensive treatment. New drugs and new drug combinations are being tested for patients with recurrent cancer. Stem cell transplantation is being studied as a strategy for helping men with poor prognosis tumors tolerate more intensive chemotherapy. And, chemotherapy combinations are being refined to see if eliminating certain drugs, replacing them with others, or lowering doses can reduce side effects for some men without reducing the effectiveness of treatment. Recent studies have found that men who are HIV-positive have an increased risk of developing testicular cancer and that most of these men can be cured using standard treatment (orchiectomy, chemotherapy, and/or radiation therapy) and can experience an improved quality of life despite their HIV status. Source: American Cancer
Society, www.cancer.org
800.ACS.2345 A Note from
a Surfer Years ago I discovered I had two and a 'half' testicles. It was about the time when the famous UK jockey Bob Champion discovered he had testicular cancer. I can tell you I was alarmed. Within hours I had seen my doctor, the next evening a specialist. He saw me privately in an evening and came at me in a darkened room with a torch light - apparently something to do with the transparency of the swelling. Six weeks later I had an epidermal cyst removed, plus a check-up on the other side too - a lab test showed it was not malignant. Any lumps anywhere now are checked out fast. The earlier a patient male or female gets attention the better. Sadly my wife had one that did not make itself noticed until quite by accident - annual eye examination - pressure - urine test - Physical - What this? She goes into hospital for a big operation on the 19th August. Mine was bad enough and when I came round I was bandaged from hip to navel I thought the lot had gone. But no! The early discovery ensured we got it before too much damage. I still have a husky voice! Menstuff - Do keep up the good promotion - It could save a surfer from really serious ill health or even loosing his prize jewels. Stan Clare, Preston, United Kingdom. Addendum: A word of warning though to all readers. Sometimes your medical advisors get it wrong - If a problem persists, get another opinion. Even then make sure the new advisor starts from scratch. If all they are going to do is look at your notes and concur, with possible bias - the easier way - then this is a waste of time. Take my 10 weeks of back ache, heavier and heavier pain killers - Three doctors declared sciatica - then ultimately the best - 'This sciatica will eventually go out through your feet!' Bollocks in my case it was 'something else! One weekend an emergency doctor no. 4 (with no medical notes!) diagnosed 'an infected prostrate' and gave me two special antibiotic pills. Within 24 hours I was up and about for the first time for nine weeks. The original doctor dashed to my home with a colleague the next morning. They were really concerned at the new concept, especially my almost instant recovery - 'We'll continue on the antibiotics. Get you right again. Then GET TESTS DONE!' - To see what damage had been done - Fortunately none. In the United Kingdom the population
has the National Health Service available - often maligned
but fantastic all in all. Totally free to residents after
you reach 60. Sometimes you have to wait for treatment
however private work is reasonably priced. The internet has
opened up new possibilities though and medical treatment can
be sourced privately in other countries at bargain prices,
quicker too sometimes. A Man Took A
Pregnancy Test As A Joke And Ended Up Finding Out Something
Awful You probably never thought you’d read about men taking pregnancy tests, but it’s now happening around the world—for a good reason, too. It all started out as a joke, but what happens when the punchline ends up being something incredibly serious? When one man decided to take a pregnancy test he found in his medicine cabinet, he never expected the result to be positive. The real surprise, though, is that the positive result wasn’t just a mishap, a faulty test, or a joke from an evil pregnancy test manufacturer. No, for this man, the positive result actually meant something. Taking a pregnancy test can fill people with a wide range of emotions—happiness, sadness, excitement, fear, hope. Some take them hoping for a positive result after months of negatives, while others take them praying to see a single line instead of two. No matter the person’s situation, however, there’s usually one thing all pregnancy tests have in common: they’re taken by a woman. Why would a man take a pregnancy test? Most of us would guess it’d be out of sheer curiosity about what would happen, on a dare from a friend, or just for a laugh while you’re bored. The latter is exactly why one man said his friend took a pregnancy test. He found it in a cabinet from his ex-girlfriend who had moved out. No big deal—at least they never had a pregnancy scare to deal with, right? Unfortunately, this little joke, which the man thought would turn out to just be a funny story, turned out to be a lot more than what he bargained for. And imagine how shocked he was when it came back positive! A positive pregnancy test is usually a happy time. Surprise or not, most women are excited about the new life developing. This man, though, has a different story to tell. And after he shared the story on Reddit, men across the world are now taking pregnancy tests as well. Why? To screen themselves for something no man wants. Let’s go back to the beginning: It all started off innocently enough. A Reddit user, who has since deleted his account, decided to make a crudely drawn comic about his male friend’s decision to use a pregnancy test. The test had apparently been left behind in his medicine cabinet by his ex-girlfriend, so he decided to give it a try for a laugh, thinking nothing would really happen. Much to their surprise, however, the test came back positive. The two clearly didn’t think the positive result meant anything, but thought the outcome was hilarious nonetheless, so they decided to use it to gain some karma on Reddit. What they got, though, was tons of advice that actually ended up saving the life of this user’s friend. After the comic was posted, comments flooded in that suggested whoever took the test needed to see a doctor immediately. There were so many that he decided the advice couldn’t be ignored, and the friend went to the doctor shortly after. Believe it or not, doctors actually detected a small tumor in the friend’s right testicle—because it was caught so early on, it was small enough that it hadn’t spread to any other areas of his body and could be treated right away. The Reddit user later posted a follow-up comic to thank everyone for giving him the advice that saved his friend from a much worse fate. He urged other men to check themselves for testicular cancer regularly, and reminded women to give themselves at-home screenings for breast cancer every now and then, too. But how, exactly, did a pregnancy test detect testicular cancer? As it turns out, it’s all about the hormones. Pregnancy tests are designed to detect the presence of a very specific hormone in the urine known as beta human chorionic gonadotrophin (hGC), which is produced during pregnancy. Though you’d probably never expect it, there are quite a few varieties of testicular cancer that also produce that very hormone—aside from testicular cancer and pregnancy, there aren’t really any other reasons why this hormone would appear in the body. According to the American Cancer Society, however, men shouldn’t rely on a pregnancy test to tell them if they have testicular cancer or not. As with women, false positives are always possible, and there’s always a chance that men with testicular cancer aren’t producing enough of the hormone for a pregnancy test to pick up. Though it might feel a little strange to follow the advice of someone on Reddit, he was correct in telling men to screen themselves for the disease often. And yes, that means self-exams. Don’t know what we’re talking about? Read on. While performing a self-exam for testicular cancer might feel a little awkward at first, it’s a necessity for men of all ages. That’s right—testicular cancer can affect men of all ages, not just those who are middle-aged or elderly. Fortunately, it’s a disease that’s usually easy to treat and cure, especially when you discover it early on. It’s best to perform a self-exam right after you get out of the shower of bathtub, so that the skin in your nether region is softer and more relaxed. You’ll take one testicle at a time gently roll it between your thumbs and fingers, using both hands. You’ll be feeling for any hard lumps or bumps, abnormal swelling or changes in size, and areas that feel thicker than the rest. Rest assured, though—it’s not abnormal for one testicle to be larger or for one to hang lower. Once you begin checking yourself regularly, it’ll be easier to tell what feels normal for you so you’re aware of any changes. Finding a lump on one of the testicles is what most people think of when they think of testicular cancer, but there are other signs to look out for, too. Unfortunately, a lot of them might now show up until the cancer is advanced, but it might not show many symptoms even then. The additional signs you need to look out for include:
If your cancer has spread beyond the testicles, you can also develop other symptoms that will vary based on where the cancer has spread.
For any women out there wondering if pregnancy tests can detect anything other than pregnancy in women, the answer is actually yes. Though ovarian cancer is somewhat rare in the United States, it’s also possible that a pregnancy test could detect the presence of this type of cancer in a woman’s body. It would do so in the same way that it would for testicular cancer in men—by picking up on the presence of beta hGC produced by the tumor. The only obvious caveat for women is that a positive pregnancy test could also very well mean there’s a pregnancy happening so, if you find out you’re not pregnant after a positive pregnancy test, the threat of ovarian cancer is worth exploring. We all know, however, that false
positives are a thing, so it really is best to just discuss
the outcome with your doctor before you assume the
worst. Ignoring
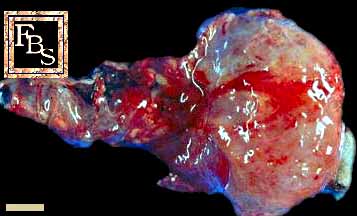
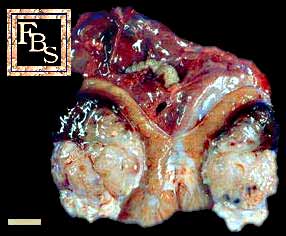
Testicular Lumps Can Cause Unnecessary Deaths: Young Men
Need to Get Medical Help Early Testicular cancer that has spread to other parts of the body has a high rate of cure (more than 80%). And even those who have a type of high-risk disease can be easily cured if caught early. In a case reported by H. D. de Boer, MD, and colleagues at the University Medical Centre in St. Radboud, the Netherlands, a 17-year-old man died in a car accident, and it was later discovered that he had testicular cancer. His medical history showed no abnormalities, and except for complaints of abdominal pain after the accident, he had been without any symptoms, de Boer said. Overlooked Tumor Found In trying to learn of the cause of the young man's death, doctors found a large tumor of the right testicle. His cancer had spread to the liver, bone, and other areas of the body, De Boer said. They found that a blood clot that reached his lungs caused his death. The authors believed the delay in diagnosis may have been due to the patient's lack of knowledge, embarrassment, ignorance, or fear of cancer. "This tragic case reminds us…early recognition of testicular carcinoma is essential," said the authors. It has been shown that treatment delay of more than three months, de Boer said, is linked to shorter survival rates. The lump had probably been noticeable for months, according to Jeremy P.C. Steele and R. Timothy Oliver, medical oncologists at St. Bartholomew's Hospital in London, who commented on the case in the same journal. Self-Exam and Proper Medical Exam Vital Such cases are not exceptional, they said. In their experience they treat about 50 new patients with testicular cancer each year, and four of these have huge testicular masses that have been hidden for months. They said that no single reason is given, but some patients admit to being afraid of seeing doctors, and in some, the family doctor said nothing was wrong. Steele and Oliver said doctors should teach men to check for testicular lumps, and when spotted, know that they are a medical emergency. The Dutch authors agreed: "It is
important to encourage testicular self-examination and to
emphasize the need for prompt medical advice in the event of
change in a previously normal testicle." The dead might as well try to speak to the living as the old to the young. - Willa Cather |
{kind=link}
{kind=link}
{kind=link}
{kind=link}